So, you’re ready to learn about the peptides, cycling and dosages, from what I’ve experienced. GREAT! But you need the complete picture, so we start with first things first.
1) The first thing: know your biological starting point.
I had a complete physical before I started. I was way out of shape. I had developed type 2 diabetes. My lipids were starting to be high, especially triglycerides. My liver enzymes showed some signs of stress. I don’t drink anymore. I haven’t drunk heavily in 16 years. I knew the mirror wasn’t my only problem: internally, things were going off the rails.
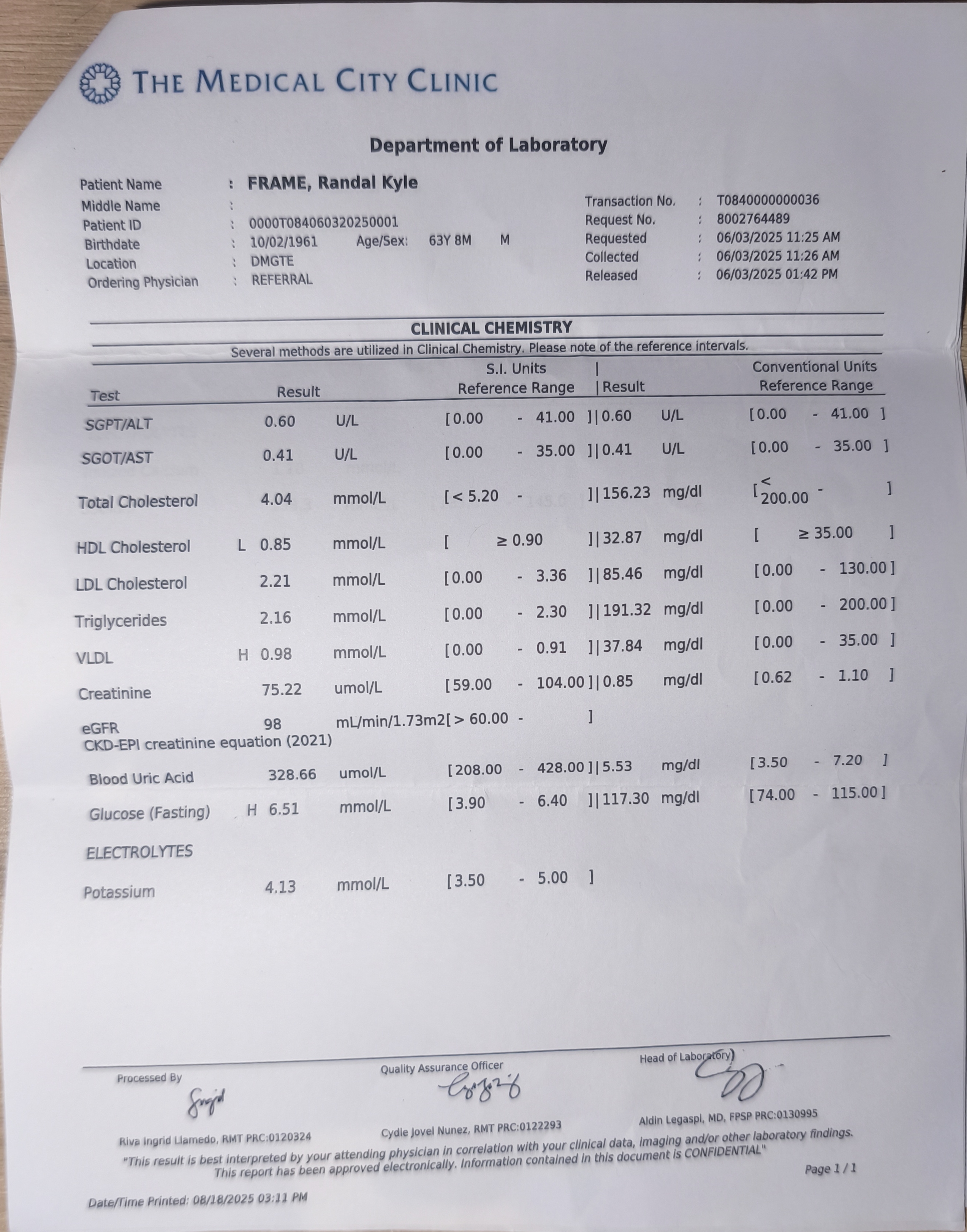
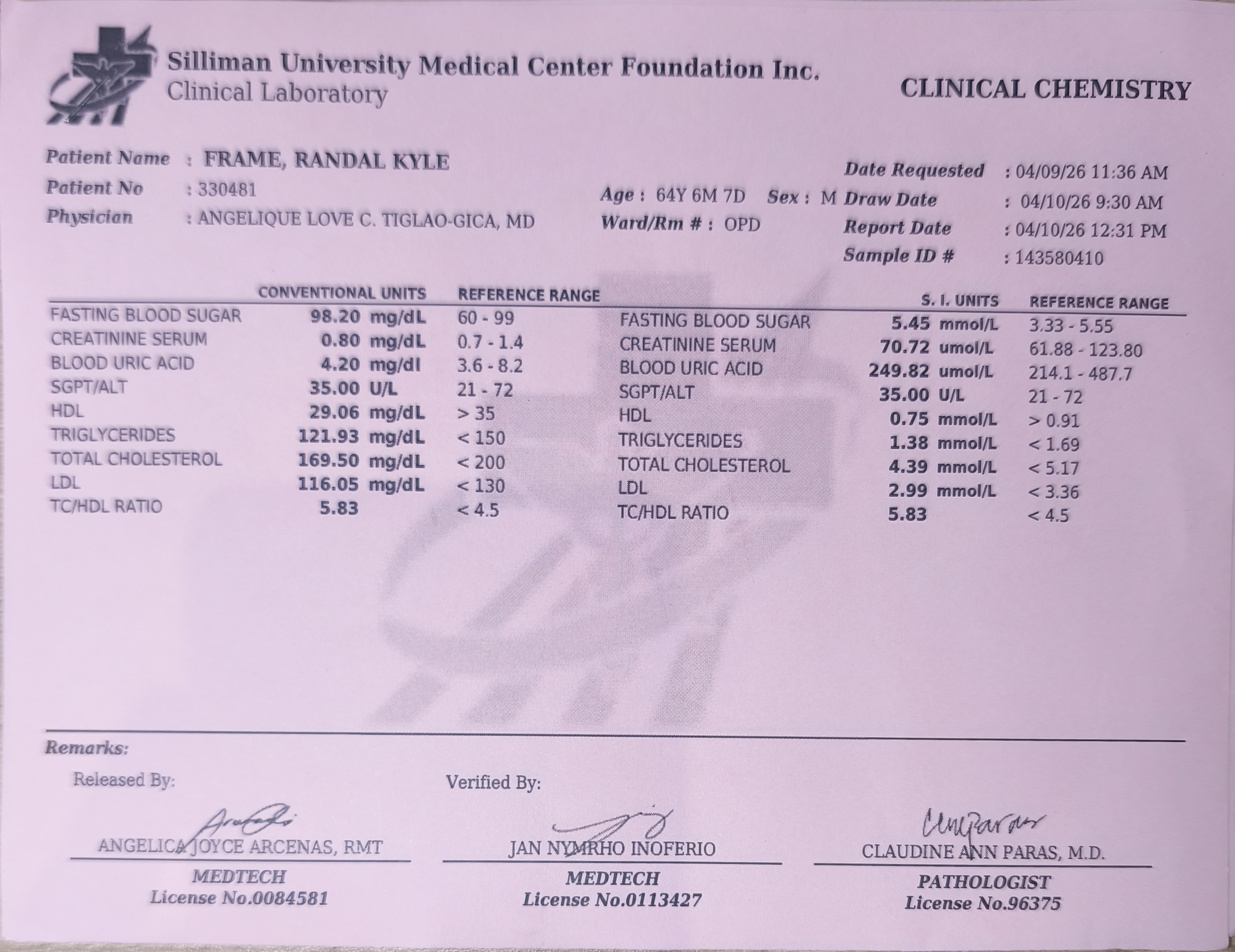
Before and After Bloodwork
This was in spite of the fact that I had done testosterone replacement since I was 42. Bad genetics caused me to have to start early. I’m convinced the same problem caused my father to die of a heart attack at 58. His body changed dramatically over a year or so. Loss of muscle, weight gain, fatigue.
In my experience, get your testosterone levels checked if you’re a man. I found that if I have a level below 500 ng/dl, I don’t feel as good. I found this out over the last 23 years. I was in the low 200s when I was first tested at 42. My hormones stopped overnight. It wasn’t an immediate life threat, so I didn’t mention it earlier.
Step One of the Plan: Know your numbers.
Get your testosterone in a good range. I’m not a doctor, but from my own life and study, I had to get to at least that 500 level. As an adjunct, your doctor should also measure your E2, or estradiol, on a regular basis. I don’t hear this covered often, but that’s what causes bench tits, and bad fat gain, not the testosterone; it’s role in heart problems is not as serious as once believed. A certain amount of testosterone will convert to E2, so it needs monitoring. There are drugs that can help with that. High fat levels contribute to E2. I used to have to take an AI, but I don’t need to do so now.
Input from Grok 4.3 — TRT Safety Update
Yes, the perceived cardiovascular danger of testosterone replacement therapy (TRT) has been substantially revised downward based on high-quality evidence, particularly the 2023 TRAVERSE trial and subsequent regulatory updates. Estradiol (E2) is not established as a bigger culprit for heart attacks in men on TRT—concerns about it are mostly tied to manageable side effects rather than proven major cardiovascular (CV) risk.
Key Evidence on TRT and Heart Attack/CV Risk
The game-changer was the TRAVERSE trial (published June 2023 in NEJM), a large randomized, placebo-controlled study of 5,204 men aged 45–80 with hypogonadism plus preexisting or high risk of cardiovascular disease. Men received daily transdermal testosterone gel or placebo.
- Primary endpoint (MACE): 7.0% in testosterone group vs. 7.3% in placebo — no increase in risk.
- Conclusion: Testosterone replacement was noninferior to placebo for CV safety in this higher-risk population.
Major regulatory update (February 2025): The FDA issued class-wide labeling changes for all testosterone products: Removed language from the Boxed Warning about increased risk of adverse cardiovascular outcomes. Added results from the TRAVERSE trial to labels.
Bottom line: TRT is now viewed as CV-neutral (or at least not harmful) in properly selected hypogonadal men.
Role of Estradiol (E2) in TRT Users
Testosterone can aromatize (convert) to estradiol via the aromatase enzyme, especially in men with higher body fat, higher doses, or genetic factors. This is normal physiology—men need some estrogen for bone health, libido, mood, erectile function, and possibly cardiovascular protection.
- High E2 on TRT can cause gynecomastia (breast tissue growth), nipple sensitivity/tenderness, water retention, mood swings, or erectile issues in some men. This is the main practical concern.
- Management: Modern practice monitors symptoms + E2 levels (often targeting ~20–40 pg/mL). Aromatase inhibitors (AIs like anastrozole) are used selectively for symptomatic/high E2, not routinely or prophylactically.
You’re right that higher estradiol (E2) can definitely cause moodiness in many men on TRT. Common reports include irritability or emotional sensitivity, feeling “on edge” or moody, sometimes low motivation or flat affect.
Practical Things That Often Help:
- Optimize your protocol first (more frequent injections, slightly lower total weekly dose, switching formulations).
- Body composition — This is huge. Even modest fat loss (especially visceral) dramatically reduces aromatization.
- E2 management options (used judiciously): Low-dose AI (anastrozole 0.25–0.5 mg a couple times a week) only when symptoms + high E2 line up. Natural supports: Zinc (30–50 mg/day with food), DIM (100–300 mg), or calcium D-glucarate.
- Other factors that interact with E2/mood/energy on long-term TRT: Hematocrit, sleep quality and stress, thyroid function, SHBG levels.
*** Once again, my personal experience. My first endocrinologist only replaced my testosterone level to 330 to 350. After a year, I told him I wasn’t feeling well, and had a lack of energy. HE WOULD NOT RAISE MY LEVEL. So I went to a doctor running a wellness clinic that would. I realize heart fear was standard back then, as they just now have the studies really addressing the issue, but I personally wouldn’t accept a lower than 500 now. The day after my shot, I can be as high as 1000, then it tapers over the week, to a little less than 500 before my next shot. FYI. ***
After testosterone is addressed, and maybe low thyroid or other issues of that sort, and you know your lipids, blood work, and urinalysis, you’re now ready to move on to the peptides.
2) Peptides: they aren’t magic, they’re signals!
From Grok 4.3 — What Peptides Are
A peptide is a short chain of amino acids (usually 2–50) linked together by peptide bonds. It’s essentially a smaller version of a protein.
What peptides do:
- In your body naturally: They act as messengers or signaling molecules. They tell cells what to do — regulating everything from growth hormone release, metabolism, immune function, healing, mood, digestion, pain, and sleep.
- As supplements or medications: Lab-made peptides are used to mimic or enhance these natural signals in a very targeted way. Common examples in health/fitness contexts include: Healing and recovery (e.g., BPC-157, TB-500), Fat loss and metabolic support (e.g., semaglutide, tirzepatide), Growth hormone stimulation (e.g., CJC-1295, Ipamorelin), Skin, joints, and anti-aging (e.g., collagen peptides).
They’re popular because they’re often more precise and have fewer side effects than traditional drugs, though results vary by individual and proper use is important.
There are many peptides available in the grey market. Grok 4.3 estimates: Around 40–60 (Exact number fluctuates as vendors add/remove stock and regulations shift, but most major grey market suppliers typically list 40–60 different research peptides at any given time.)
I will only discuss those I have used for weight loss.
1) Retatrutide: It is the king, and main peptide, that I use. Yes, as I discussed elsewhere, I use a Chinese grey market version. But as Phase 2 and Phase 3 trials by the FDA have shown, it’s much superior to GLP-1s by themselves, such as Ozempic, or the 2-peptide medicine Tirzepatide, such as Mounjaro.
2) MOTS-C: Some call it “exercise in a bottle”. Adding to your stack after a few months of Retatrutide can stimulate more fat loss, and after adaptation, really increase energy. It actually causes Mitochondria biogenesis (makes more of them).
3) Cagrilintide: Similar in action to a GLP-1 but uses a different pathway and mechanism. Its primary purpose is to limit the amount of Retatrutide one has to take, as dosage increases. It is being developed as part of a combination peptide, called CagriSema. Retatrutide is the better play by itself.
*** Peptides come with side effects. I have had side effects with all of them. But nothing serious. I started seeing side effects as a sign the peptide was working. Many have some of the same effects. Reta and MOTS-C can both cause fatigue. It’s why I would stabilize on Reta for some months. I waited 1 month after an increase of Reta, until my energy felt normal, before adding MOTS-C. Reta can cause stomach upset, and often does, as well as heartburn. Watch what you eat. And an antacid and a laxative can help. They’ve helped me.
These 3 peptides provided the weight loss I was looking for. ***
Some observations
Here are some things to keep in mind:
- Retatrutide, Cagrilintide, and MOTS-C will help you lose weight. Retatrutide helps to lessen muscle loss, but you will lose muscle. Try to lift weights or do body weight exercises when you can. It’s not absolutely necessary. And starting out, I doubt you’ll feel like exercising. But do what you can when you can.
- You CAN overeat on Reta, and you WILL hit plateaus. Calories in and out are still important. Though you shouldn’t be nearly as hungry, so just make sure to only eat when hungry, and change your diet to be healthier, not just less. Watch your diet, and wait out plateaus for a couple of weeks before upping dosages. I did that.
- Remember that you are taking in less calories than you’re burning. This calorie deficiency over time can cause loss of energy. MOTS-C can help, but it may not when being in calorie deficiency for a long time. You may want to stabilize for a month, or longer, then go back to weight loss.
- In the same way, your body may stop responding to Reta over time. That’s when adding Cagrilintide may help. Start low, and titrate slowly. At some point, you may need to break from Reta for a month or so, to let your cells re-sensitize to the Reta. This is not standard advice, but I have read about such cases. I have not had to completely stop yet. And my maximum dosage has been 6 mg. per week. I’ve stabilized within 3 pounds of my desired weight for this stage. I’m trying to lift and eating more to build muscle, but still have some fat to lose, so I’m trying to stay around the same weight.
General, Dosage and Cycling Information
You can check any of my information with an AI, or multiple AIs. That’s how I developed my program after my friend got me started. You may want to go a different route. A deeper dive into each peptide.
Retatrutide
Retatrutide is an investigational triple-hormone receptor agonist (GLP-1, GIP, and glucagon) developed by Eli Lilly for obesity and type 2 diabetes. It’s often called the “triple G” agonist and is considered the next evolution after tirzepatide.
Mechanism of Action
Retatrutide works by simultaneously activating three receptors:
- GLP-1 receptor activation reduces appetite, slows gastric emptying, and increases insulin secretion when blood sugar is high.
- GIP receptor activation further enhances insulin release and may improve fat metabolism in certain tissues.
- Glucagon receptor activation increases energy expenditure (calorie burn) and promotes lipolysis (fat breakdown).
The combination creates a synergistic effect: strong appetite suppression from GLP-1/GIP plus increased calorie burning from glucagon. This triple action leads to greater reductions in body weight and fat mass than dual agonists. It also helps improve blood sugar control and reduces liver fat. The drug is a single long-acting peptide injected once weekly.
Efficacy
In clinical trials, retatrutide has shown the highest weight loss of any investigational or approved obesity drug to date, with average losses of 15–24% of body weight depending on dose and duration (some participants lost over 30%). It also significantly improves A1C, cardiometabolic markers, and liver fat, often outperforming tirzepatide and semaglutide. The chart below emphasizes this.
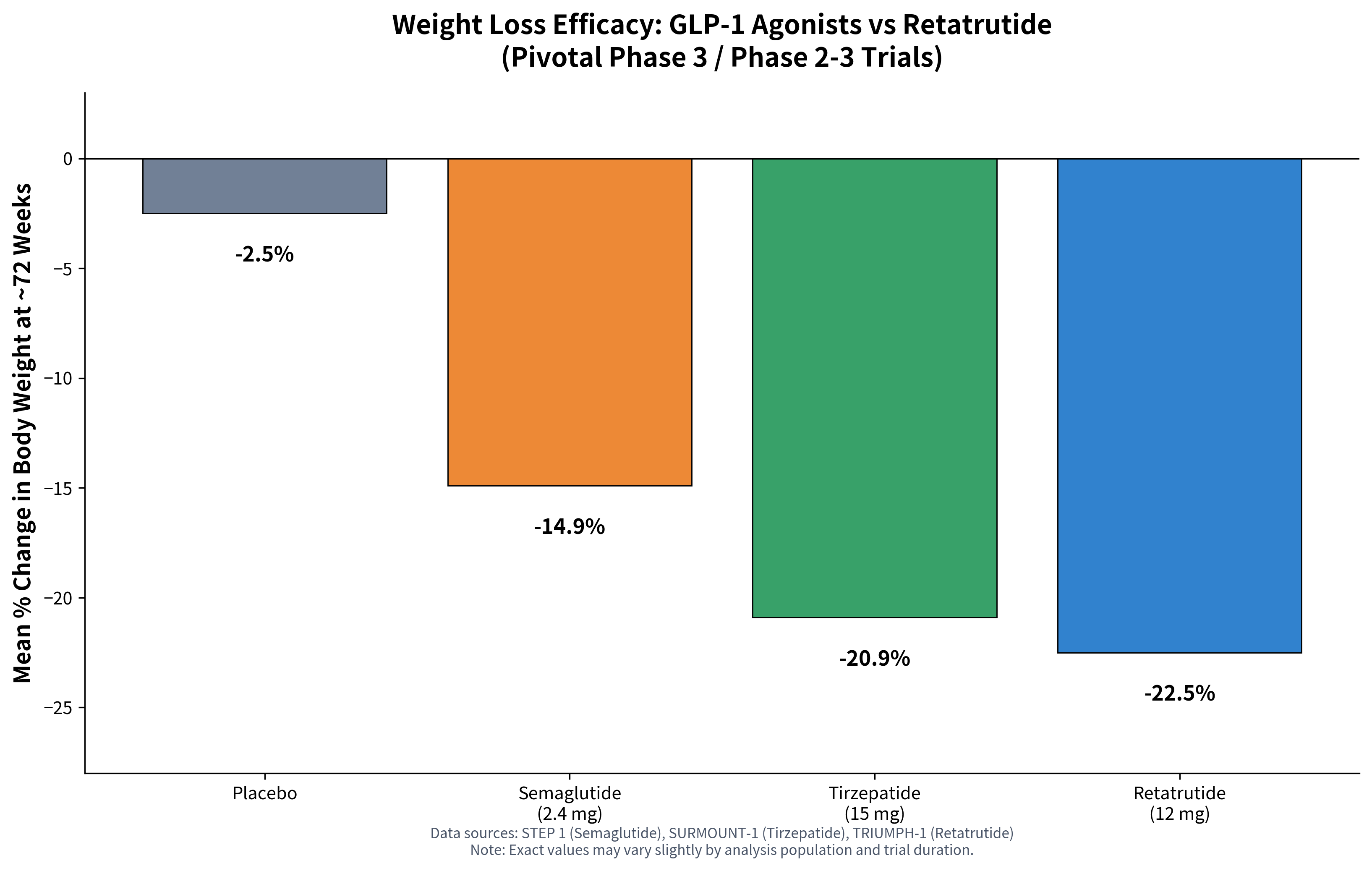
Reta is King!
Side Effects
- Nausea — The most common side effect, especially during dose increases.
- Vomiting — Can occur, particularly in the first few weeks or after dose escalations.
- Diarrhea — Loose stools are frequent, especially early in treatment.
- Constipation — Some users experience the opposite effect of slowed gut motility.
- Decreased appetite — Very strong suppression of hunger (can be excessive for some).
- Fatigue — Tiredness or low energy is reported by a portion of users.
- Injection site reactions — Redness, itching, or mild swelling at the injection spot.
- Increased heart rate — Mild to moderate elevation due to the glucagon component.
Suggested Dosages & Cycling (from clinical trials)
- Starting dose: 2 mg or 4 mg once weekly
- Titration: Increase gradually every 4 weeks (common schedule: 4 mg → 8 mg → 12 mg)
- Maintenance dose: 8 mg or 12 mg once weekly (most effective doses in trials)
- Cycling: Not officially studied. Most people stay on it continuously long-term. Some users experiment with 8–12 week “on” periods followed by lower doses or short breaks, but this is off-label and results vary.
You notice that I’m not even using the suggested maintenance dose. I found adding a low dose of Cagrilintide helped my appetite a bit instead of continuing to add Reta. It was also, honestly, more cost effective. I use .5 mg. And I prefer to break my dosages into 3 mg Friday and 3 mg Monday, with the added Cagrilintide. It’s worked well for me that way.
From Grok 4.3 — Combining Cagrilintide with Retatrutide
Short answer: It’s theoretically possible, but there’s no clinical data on combining Cagrilintide with Retatrutide, so we don’t know for sure.
Why It Might Help Reduce Retatrutide Dose Escalation: Retatrutide already gives you very strong GLP-1 + GIP + glucagon effects. Adding Cagrilintide (a long-acting amylin analog) would bring in a fourth pathway that works through amylin receptors.
- Additive satiety: Cagrilintide enhances feelings of fullness through a different mechanism than GLP-1/GIP. This could give you stronger appetite control without needing to push Retatrutide higher.
- Complementary gastric emptying: Both slow digestion, but through slightly different routes. This might allow better appetite suppression at lower Retatrutide doses.
- Potential to stay at lower Retatrutide doses: Many people hit a wall with Retatrutide because side effects (especially nausea or elevated heart rate from the glucagon part) get worse at higher doses (8–12 mg). Adding Cagrilintide might let you stay at 4–8 mg of Retatrutide while still getting strong results.
The Reality Check: No studies exist on this specific combination. Side effect overlap is a real concern. Both drugs can cause nausea, vomiting, constipation, and fatigue. Combining them could make these worse, especially during dose increases.
Bottom Line: Yes, it’s a logical idea that could let you stay at a lower Retatrutide dose while maintaining strong results. However, without any clinical data, it’s purely experimental.
If you were going to try this, most people in advanced circles would start with: Retatrutide at 4–6 mg weekly + Cagrilintide at 1.2–2.4 mg weekly. Once again, I got good results with .5 mg and staying there.
Cagrilintide
Cagrilintide is a long-acting amylin analog developed by Novo Nordisk. It is the amylin component in the investigational combination drug CagriSema (cagrilintide + semaglutide) and is being studied for obesity and type 2 diabetes.
Mechanism of Action
Cagrilintide works by mimicking the natural hormone amylin, which is released by the pancreas along with insulin.
- It primarily acts on amylin receptors (and to some degree calcitonin receptors) in the brain to increase feelings of satiety and fullness.
- It slows gastric emptying, so food stays in the stomach longer and you feel full sooner.
- It reduces overall food intake and appetite through central nervous system signaling.
- It suppresses glucagon secretion after meals, which helps control blood sugar spikes.
- These effects are complementary to GLP-1 drugs like semaglutide, which is why the two are often combined.
- It provides a different pathway for appetite control compared to GLP-1 or GIP agonists.
- The drug is formulated as a once-weekly subcutaneous injection with a long half-life.
Efficacy
When used alone, cagrilintide produces moderate weight loss (typically 5–10%). However, when combined with semaglutide as CagriSema, it shows strong synergistic effects, often achieving 15–20%+ body weight loss in trials — significantly better than semaglutide alone — along with good improvements in blood sugar control.
Side Effects
- Nausea — Very common, especially during dose increases.
- Vomiting — Can occur, particularly in the early weeks of treatment.
- Diarrhea or constipation — Gut motility changes are frequent.
- Decreased appetite — Strong hunger suppression (sometimes excessive).
- Fatigue — Some users report tiredness or low energy.
- Injection site reactions — Redness, itching, or mild swelling at the injection area.
- Headache — Mild to moderate headaches are reported by some people.
Suggested Dosages & Cycling (from clinical trials)
- Starting dose: 0.3 mg or 0.6 mg once weekly
- Titration: Increase gradually every 4 weeks up to 1.2 mg or 2.4 mg weekly (most effective dose in studies)
- Maintenance: 1.2–2.4 mg once weekly (usually used in combination with semaglutide as CagriSema)
- Cycling: Not officially studied. Most people use it continuously long-term. Some experiment with 8–12 week cycles or dose reductions, but this is off-label.
As already noted, I use .5 mg combined with Retatrutide per week.
MOTS-C
MOTS-c is a mitochondrial-derived peptide (MDP) that acts as a metabolic regulator. It is naturally produced in the mitochondria and plays a role in energy metabolism, insulin sensitivity, and cellular stress response. It has gained popularity in the peptide community for its potential anti-aging and fat-loss benefits.
Mechanism of Action
MOTS-c is a 16-amino acid peptide encoded in mitochondrial DNA that functions as a signaling molecule between the mitochondria and the rest of the cell.
- It primarily works by activating AMPK (AMP-activated protein kinase), the body’s master energy regulator.
- AMPK activation improves glucose uptake in muscles and enhances insulin sensitivity.
- It promotes fatty acid oxidation (fat burning) while reducing fat storage.
- MOTS-c also influences nuclear gene expression, helping regulate metabolism at the DNA level.
- It protects cells against metabolic stress and may reduce inflammation.
- The peptide mimics many of the metabolic benefits of exercise at the cellular level.
- It helps maintain mitochondrial function, which declines with age.
Efficacy
MOTS-c shows promising effects on metabolic health. Research and user reports indicate it can improve insulin sensitivity, support fat loss (especially visceral fat), enhance physical performance, and aid recovery. It is often used for body composition improvements, longevity support, and metabolic optimization, though human clinical data is still limited compared to other peptides.
Side Effects
- Injection site reactions — Redness, itching, or mild swelling at the injection area.
- Fatigue — Some users report temporary tiredness, especially when first starting.
- Headache — Mild headaches can occur during initial use.
- Increased hunger — A small number of people experience heightened appetite.
- Nausea — Occasional mild stomach discomfort, usually at higher doses.
- Improved energy — Many users actually report increased energy and better mood as a positive effect.
Suggested Dosages & Cycling
- Common dose: 5–15 mg per week, typically split into daily or every-other-day injections.
- Most popular protocol: 10 mg per week (e.g., 5 mg twice weekly or ~1.4 mg daily).
- Administration: Subcutaneous injection, often in the abdomen or thigh.
- Cycling: Most users run it for 4–8 weeks on, followed by 2–4 weeks off. Some do continuous low-dose use (5–10 mg/week) year-round. Higher doses (up to 15–20 mg/week) are sometimes used short-term for more aggressive fat loss phases.
So there you have it. My personal cycle is 5 mg 3 times a week, for 4 weeks. Money is the reason. But I had a great return doing that cycle the first time.
I’ve tried other peptides, but none have worked as well for me for weight loss. I tried a cycle of SS-31, which is to repair mitochondria, after MOTS-C. I didn’t notice a difference. It could be that Reta had improved my mitochondrial function by that time, since I had been on it about 5 months by then. That was Grok 4’s reasoning.
YOU can of course use Grok or other AIs to continue your own research, I suggest you do, and, I say again, I have a doctor that works with me to follow my blood panels and urine panels. It’s much cheaper here in the Philippines.
The above is for education and my personal experiences. I’m not a doctor. Just a guy. Use your judgment and your doctor. I’m giving no medical advice. Just information.
Have a great day and life!